
Antithrombotic Therapy
New Oral Anticoagulant and Antiplatelet Drugs
President Message
Part II
(January 2022)
M. Mohsen Ibrahim, MD
Antiplatelet Drugs
ROLE OF BLOOD PLATLETS
Form a platelet plug or thrombus to prevent blood loss when a blood vessel is injured. They are the first hemostatic mechanism.
Platelets normally circulate in blood as inactive tiny discs (2-3 microns in diameter) without nuclei and have smooth cell membrane which is very rich in platelet receptors.
When endothelium is injured or disrupted with exposure of the sub-endothelial matrix proteins and cells, adhesion proteins mainly collagen and von Willebrand factor adhere to platelets leading to platelets activation.
Platelet activation results in: (1) change in platelet shape from smooth discs to spiny spheres, (2) secretion of platelet contents such as serotonin, ADP, arachidonic acid, thrombin, fibrinogen, and adhesion proteins, (3) exposure and activation of GP IIb/IIIa receptors which are fibrinogen receptors. Fibrinogen forms cross bridges between activated platelets resulting in formation of platelet aggregates.
In the absence of cardiac arrhythmias and valvular heart disease, prevention of coronary thrombosis mainly relies on antiplatelet therapy.
Antiplatelet Drugs
– Aspirin
Inhibits cyclooxygenase enzyme (coxi), an enzyme responsible for the generation of thromboxane. Coxi converts arachidonic acid into the prostaglandin GZ, a precursor of prostaglandin PGH2.
PGH2 is either converted into prostacyclin-by-prostacyclin synthase present in endothelial cells or converted into TXA2 by thromboxane synthase in platelets.
Low dose aspirin inhibits platelet synthesis of thromboxane, while maintain endothelial synthesis of prostacyclin.
In addition to antiplatelet activity aspirin reduces markers of inflammation.
– P2Y12 Inhibitors: Thienopyridines:
Clopidogrel – Prasugrel – Ticagrelor
Block the binding of adenosine diphosphate (ADP) to a specific platelet receptor P2Y12.
Thienopyridines indirectly inhibit the activity of other platelet agonists such as arachidonic acid, collagen, thrombin, epinephrine, and serotonin. Also, they inhibit platelet aggregation induced by collagen and thrombin.
Clopidogrel and prasugrel are prodrugs, while ticagrelor is an active drug with additional active metabolites. Antiplatelet potency is greatest with prasugrel and less with clopidogrel and moderate with ticagrelor.
– Clopidogrel Vs. Ticagrelor
Ticagrelor is more effective, and for patients with ACS, it quickly inhibits platelet aggregation, while clopidogrel is less effective.
Clopidogrel is a prodrug, its activation can be influenced by genetic factors with some patients have clopidogrel resistance. Its onset of action is somewhat delayed and initial large loading dose is required.
In ACS treatment with ticagrelor as compared with clopidogrel significantly reduced the rate of death, myocardial infarction, and stroke without an increase in major bleeding.
Dual Antiplatelet Therapy (DAPT)
Combination of aspirin with oral antiplatelets (Clopidogrel, Ticagrelor).
Goals of DAPT are to prevent new ischemic events and prevent stent thrombosis.
DAPT indications:
1. Post-ACS event: patients have more thrombotic phenotype, 12 months DAPT is recommended regardless of stent placement.
2. Stable ischemic heart disease is less thrombotic phenotype and DAPT is considered if a stent is placed.
3. Severe diffuse atherosclerosis, high risk patients with peripheral artery disease and cardiovascular disease specially if combined with CAD.
Clopidogrel with aspirin are given to patients with TIA or minor stroke. Treated within 24 hours after onset of symptoms. The combination is superior to aspirin alone for reducing the risk of stroke in the first 90 days.
Duration of DAPT:
– Following ACS with stent or not: 12 months.
– Stent placed in non-ACS setting: 6 months.
The ESC/EASD guidelines highlighted the superiority of modern P2Y12 inhibitors and encouraged the use of these agents for DAPT in diabetes.
Long term therapy with aspirin and ticagrelor in diabetes patients with established CAD- for a median of 33 months-reduced major adverse cardiac events beyond 12 months of the coronary event.
More studies are required to understand the best strategy for long-term antithrombotic therapy in diabetes. The enhanced thrombotic environment in diabetes calls for alternative antithrombotic treatment strategies in primary and secondary vascular protection.
Triple Therapy
Aspirin + P2Y12 inhibitor + Oral anticoagulant
Rarely indicated beyond are month duration.
P2Y12 inhibitor (clopidogrel, ticagrelor) are preferred over aspirin: NOACs are preferred over warfarin.
Continue triple therapy for maximum one month post-hospital discharge.
When transition to dual therapy drop aspirin and continue P2Y12 inhibitor.
Choose NOAC rather than warfarin unless contraindicated or cost.
When Prescribing New Antiplatelet drugs consider the following factors:
1. Potency: Prasugrel most potent, followed by ticagrelor, then clopidogrel
In the ACS setting, we tend to prefer more potent agents like ticagrelor or prasugrel in the absence of contraindications
2. Bleeding risk: Increased bleeding risk is always the tradeoff of increased potency. We avoid prasugrel in patients age > 75, history of TIA/stroke, and hepatic dysfunction Also avoid ticagrelor in patients with history of ICH
3. Feasibility- Side effects: Ticagrelor inhibits adenosine reuptake, which can cause bradycardia and dyspnea, sometimes resulting in patient self-discontinuation.
4. Dosing frequency: Clopidogrel and prasugrel are once per day, while ticagrelor is twice per day
5. Price: Clopidogrel is the least expensive.
President Massage
Hypertension – Drug treatment Strategies in Daily practice
Part II
3. How to monitor drug treatment?
Clinical evaluation and BP check are required every 2-4 month, while laboratory
monitoring for blood chemistry and ECG may be needed once / year unless there are
specific indications.
Fig 4: Initiation and Monitoring of Drug Therapy
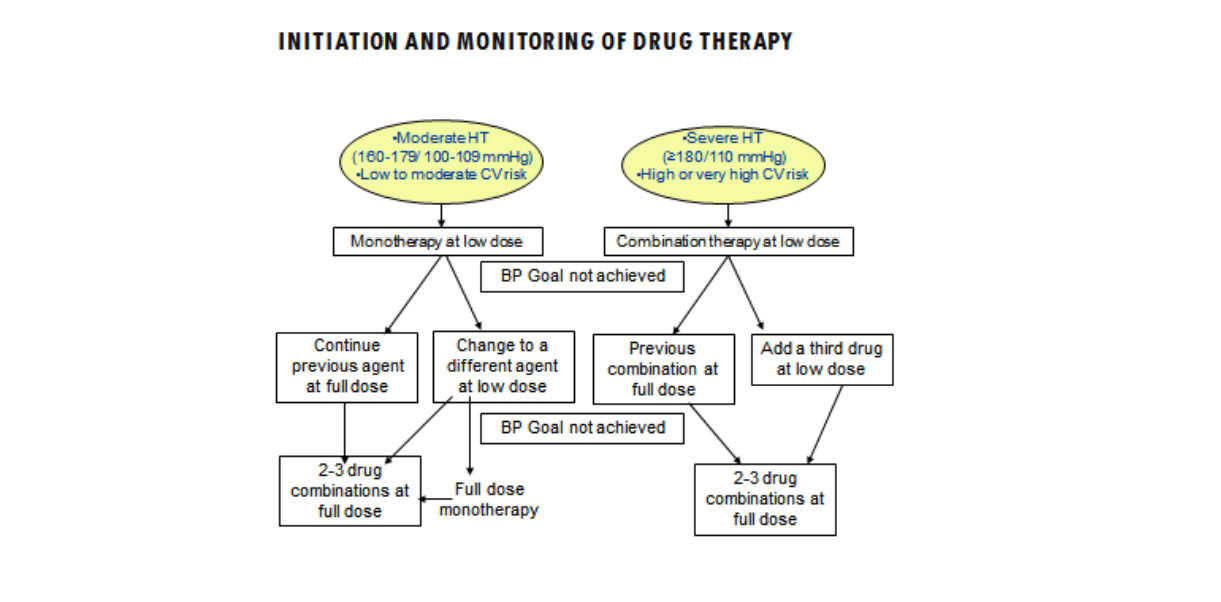
Hypertension – drug treatment strategies in daily practice. M. Mohsen Ibrahim
Antihypertensive drugs may require a period of up to two months to achieve maximal hypotensive effect. On the other hand a significant reduction in BP can be achieved after two weeks of therapy with many drugs, particularly combination therapy. It is not
recommended to change drugs at short intervals. It is advisable to recheck BP at one to two monthly interval until it remains at target level for two consecutive visits, then recheck at 3-6 months depending upon the CV risk profile. Frequency of checking BP
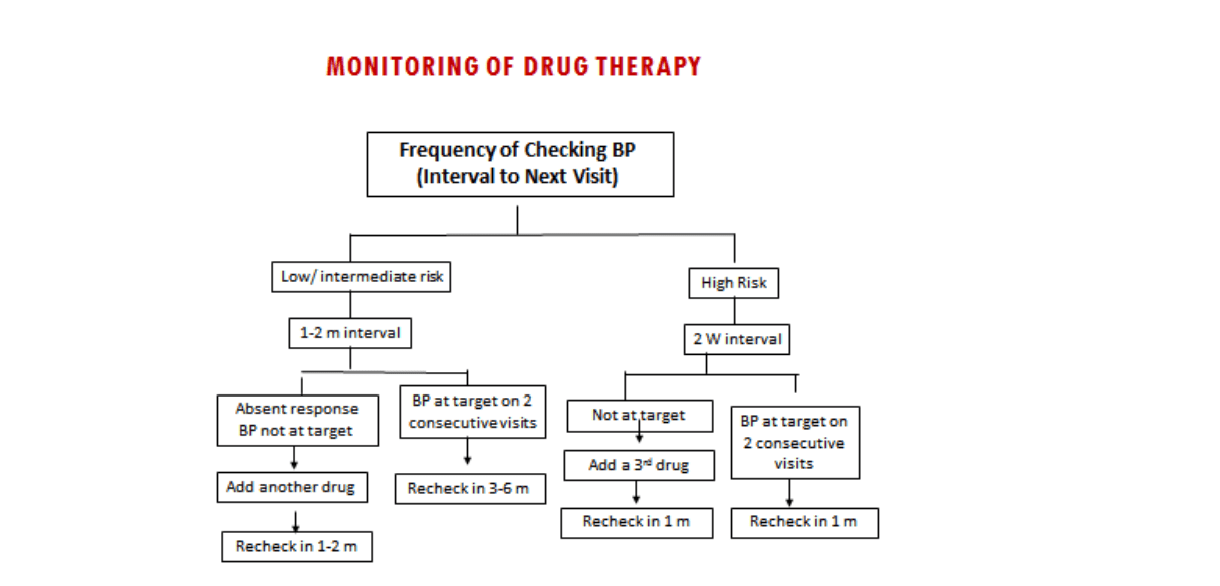
(interval to next visit) in low to intermediate risk patients is at 1-2 months intervals, while in high risk patients at two weeks intervals. Recent guidelines define BP control as < 130/80 mmHg in the office and <125/75 mmHg as determined by 24 hours ABPM
Fig 5: Monitoring of drug therapy frequency of checking BP
To improve patients compliance with antihypertensive drugs, patients education is recommended stressing the fact that HTN is silent, dangerous if not treated , requires life-long treatment and monitoring. Physician should prescribe affordable drugs while
drug administration is preferably once daily with minimal number of tablets, better a single pill combination.
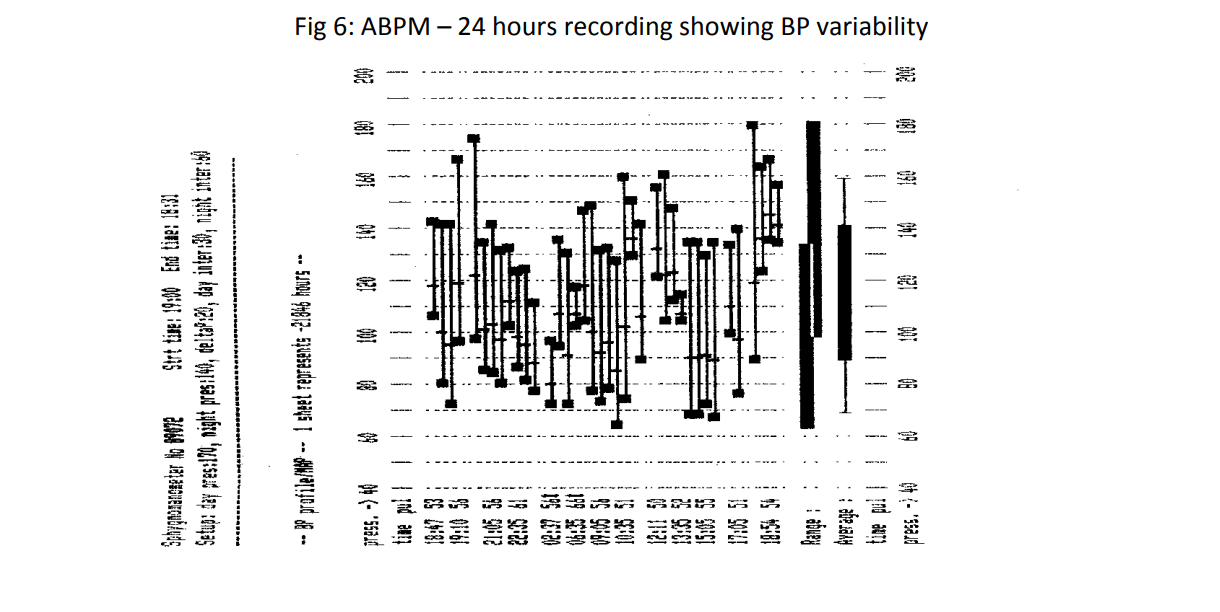
4. What to do about BP variability?
Levels of BP are liable to fluctuation and can change from minute to minute and from day to day . These fluctuations in BP can generate anxiety and confusion regarding diagnosis and treatment.
Short term BP variability may be instantaneous within seconds as occurs during sleep, pain, posture , emotions, talking, distended urinary bladder or within minutes after smoking, meals, hypoglycemia or within hours following medication or circadian-diurnal changes. Long term or office visit to visit variability can be spontaneous , due to drugs or rarely pheochromocytoma.
Guidelines regard variability of BP as noise that has to be removed from the diagnostic process and that HTN should not be diagnosed on the basis of episodic rises in BP unless mean BP is raised ( ESH 2007 guidelines). Guidelines differ regarding the management of BP variability. Some stress the need to do 24 hours ABPM or home measurements (ESH 2007), others stress the need to confirm BP elevation in 2-5 subsequent visits ( JNC, BHS and Canadian guidelines).
The treatment implication of reducing visit to visit BP variability are uncertain and there is no direct evidence that a reduction of visit to visit variability (VVV) is beneficial. However, CCBs and diuretics tend to decrease VVV, whereas BABs and RASB seem to do the opposite.
5. How to manage poor BP control and resistant hypertension?
Failure to achieve optimal BP control is responsible for 60% of cerebrovascular accidents, 50% of coronary events, for 7.1 million death/year and 64.3 million serious disabilities/ year. It is predicted that over the next 10 years health costs of non-optimal BP are likely to reach over 908 billion dollar if BP remains at current levels. Optimal BP control varied in hypertension surveys from 23% in USA, 24% in France, 16% in Canada, 8% in Egypt and 5% in China.
The causes of poor BP control may be drug, lifestyle or physician related. Drug related causes include limited access to treatment, poor adherence or inadequate,dosage. Lifestyle causes are unhealthy diet, excess salt intake, obesity, sedentary
lifestyle and continuous emotional stress. Lack of adherence to treatment guidelines, inadequate follow-up, therapeutic inertia and lack of adequate time with the patient are physician and health system related causes.
In an Egyptian survey of 1534 hypertensive patients up to 79% of patients quite treatments within the first year. Only 10-15% of originally treated patients were still adherent to treatment after five or more years.
Resistant Hypertension
Definition (AHA 2018) of resistant HTN:
Above goal BP despite 3 or more BP medications commonly including a long acting
CCB, RAS blocker and a diuretic at maximally tolerated doses and appropriate
dosing frequency, excluding white coat HTN with ABPM or home monitoring and
medication non-adherence. This definition excludes causes of false resistance.
Management of resistant HTN
First exclude pseudo-rsistance by accurate BP measurement, ensuring adherence to lifestyle modification and antihypertensive therapy. ABPM (24 hours) and if unavailable use home BP in order to exclude white-coat HTN. Also history of intake of pressor drugs and obstructive sleep apnea should be excluded, then increase the dose of diuretics since blood volume expnasion is an important cause of resistant HTN. Long acting loop diuretic is added and if fail add spironolactone.
Assess for secondary HTN if still BP is not controlled after the previous measures. Causes include primary aldosteronisne , renal parenchymal disease, renal artery stenosis, pheochromocytomar, paraganglioma, Cushing syndrome, coarctation of
the aorta and other endocrcine causes.
What to do if there is inadequate BP response?
1. Exclude :
a. Pseudo resistance and white coat effect
b. Intake of pressor drugs
c. Obstructive sleep apnea
2. Stress lifestyle modification:
a. Limiting salt intake
b. Treat obesity
c. Stress management
3. Pharmacologic treatment:
a. Blood volume control: aggressive diuresis-use loop diuretics
b. Aldactone/ spironolactone
c. BABs if heart rate is >70 b/m
d. α-blockers and vasodilators if heart rate < 70 b/m
4. If fail screen for secondary hypertension
6. What is the role of new anti-hypertensive drugs?
Many of the following drugs are not yet established standard treatment for HTN, but
may be part of the future drug therapy of HTN. The list of new antihypertensive drugs
include:
1. New calcium channel blockers
2. Endothelin antagonists
3. Combined ARB with a Neprilysin inhibitor
4. Aldosterone synthase inhibitors
5. Natriuretic peptide receptor agonists
6. Imidazole’s: centrally acting drugs with less side effects
7. Neutral endopeptidase inhibitors : inhibit metabolism of atrial natriuretic peptide .
8. Mineralocorticoid receptor antagonists.
1. New calcium: channel blockers:
Third generation CCB have less incidence of peripheral edema in hypertensive patients which improves drug persistence in treated patiens. Examples of new CCBs are lercanidipine, lacidipine and manidipine
2. Endothelin antagonists:
Because of their side effects ( headaches and fluid retention) they are only used in resistant hypertension or hypertension of renal disease.
3. Combined ARB with a Neprilysin inhibitor:
Neprilysin is the enzyme when breaks down natriuretic peptides. Sacubitril is a neprilysin inhibitor which enhances the vasodilation of these peptides. The combination with an ARB ( valsartan) is commercially available ( Entresto) which is used in treatment of heart failure and resistant hypertension.
4. Aldosterone synthase inhibitors:
LCI699 is the first orally active aldosterone synthase inhibitor for human use. It decreases plasma and urine aldosterone concentration. New compounds as potent and more selective than LC I 699 are currently being tested as treatment for mineralocorticoid dependent CV and renal disease.
5. Natriuretic peptide receptor agonists:
Increased natriuresis and diuresis, elevate plasma cyclic guanosine monophosphate and reduce systemic BP. PL- 3994 given subcutaneous with prolonged half life administered as an adjunct to standard therapy in patients with resistant HTN. It has reduced affinity for the natriuretic peptide clearance receptor and increased resistance to neprilysin.
6. Mineralocorticoid receptor antagonists:
Spironolactone has significant progesterone and antiandrogenic activity. Eplerenone is more selective MRA but is less potent. Finerenone, a non-steroidal MRA is more selective than spironolactone and more potent than eplerenone
Summary and Conclusion
Drug treatment of HTN has changed the outcome of hypertensive patients and is one of the most successful therapeutic achievements.
However, drug treatment does not provide cure for HTN, therefore it has to be continued indefinitely to maintain BP control. The first and possibly most critical question is when to start drug treatment. The answer depends upon the accurate diagnosis of HTN and the detection of other CV risk factors. The threshed for diagnosis of HTN depends upon the method of BP measurement and recommendation of guidelines. Office measurements have obvious limitations and recent guidelines do not depend upon office readings to establish the diagnosis and initiate therapy. ABPM and automated office measurements provide more accurate and reliable methods to diagnosis HTN. After deciding the need for drug treatment the next question is which drug to choose as initial therapy. This will depend upon patient’s age, drug cost, presence of target organ damage and co-morbid conditions. Drug combination therapy is recommended in the majority of patients mainly ACEIs, ARBs combined with CCBs and or thiazide diuretics. These agents are specially recommended in patients with CKD, DM, HF. In presence of CAD, BBs are the first choice. In elderly atients and in presence of isolated systolic HTN,CCBs and diuretics are drugs of first choice. BBs are recommended in presence of CAD, HF, tachycardia, anxiety, migraine and arrhythmias. Drug therapy requires careful monitoring. BP should be checked at 2-4 weekly intervals after initiation of treatment, then at 2-6 monthly intervals depending upon BP level and CV risk profile. BP variability is a
common problem and diagnosis of HTN should not be made unless the BP is persistently elevated. Failure to achieve optimal BP control is another common problem: Interruption and/or inadequate drug therapy is the main cause. Patients education is mandatory, stressing the silent nature of HTN and the need to continue drug therapy indefinitely. Doctors should be aware of the recent guidelines and the importance of single pill combination and regular BP monitoring. Management of true resistant HTN (after exclusion of white coat HTN), depends upon accurate diagnosis, lifestyle modification ( low salt) weight reduction, avoiding presser medications and treatment of obstructive sleep apnea. Increasing the dose of diuretics and use of spironolactone are recommended in truely resistant cases. Finally there is a rapidly growing list of new ntihypertensive drugs which are undergoing clinical trials and can be used as a last resort in truely resistant hypertensive patients.